This is sort of a follow-up to a
recent
post,
in which I discussed the correlation between administration of
fluoxetine, and neurogenesis in the hippocampus. In that
post, I
mentioned that skeptics of psychopharmacology are fond of pointing out
the lack of a well-defined connection between the inhibition of
serotonin reuptake, and the clinical effects of the serotonin reuptake
inhibitors.
The hypothesis that there is a connection between serotonin and
depression is a refinement of the monoamine hypothesis of depression.
That hypothesis states that there may be a connection between
relative underactivity of brain monoamines (serotonin, norepinepherine,
dopamine) and depression. It is an old idea, derived in part
from studies such as this one: Antagonism to reserpine
induced depression by imipramine, related psychoactive drugs, and some
autonomic agents
. Sigg EB, Gyermek L, Hill
RT.
Psychopharmacologia. 1965 Feb
15;7(2):144-9.
Obviously, we have learned a lot since 1965, so the monoamine
hypothesis is significant mainly as an historical relic. Even
the refinement -- the serotonin hypothesis -- is ancient.
Since then, ample evidence has been found, showing that the
serotonin hypothesis is, at best, a gross oversimplification.
There is no strict correlation between serotonin activity and
any defined mental illness.
The lack of a strict correlation means that the action of
antidepressant
medication is not fully understood; nobody I know will dispute that.
But the thing is, harping on that string is pointless. It is
like
pointing out that there is not a strict correlation between the noise
of an automobile engine, and the motion of he automobile. It
is
true that sometimes an automobile moves without the engine making
noise; and sometimes the engine makes noise without moving.
Sometimes there is a significant lag between the time the
engine
starts making noise, and the time the automobile starts to move.
With the correct instruments, it would even be possible to
show
that
none of the energy that goes into the production of noise has anything
to do with the movement of the automobile. True, all of it.
But can we conclude that there is no connection between the
noise
of the automobile, and the motion?
Perhaps the serotonin boost is not at all related to the clinical
effect. It could be an
epiphenomenon.
Physicians generally know about epiphenomena, and are
cautious about overinterpreting them. Pointing out the fact,
that there is not necessarily a causal connection, is tiresome.
Thus, when a skeptic takes pains to point it out, it merely
shows that the skeptic is not aware of how obvious it is to
medically-educated people.
As an aside, it occurs to me that epiphenomena are roughly analogous to
spandrels.
If I felt like getting tediously philosophical, I could write
a post outlining that analogy. Another time, perhaps.
(A hint: just as a feature that evolves as a spandrel can
turn out to be useful, sometimes side effects of mediation can be
useful.)
Sometimes it is difficult to avoid getting tediously philosophical.
Oh well. It occurs to me also that this is an
example of how a good understanding of evolutionary theory can be
helpful in understanding medicine, as Orac is
fond
of pointing out. (As is my former residency
director,
Randy
Nesse.) This is true regardless of whether you
believe that evolution is responsible for the origin of species.
Putting that aside aside, and getting back to the point: Because it is
tiresome to hear skeptics harp on that string (the lack of a
fully-delineated connection between serotonin and depression) I was
surprised to see this article in a well-regarded journal:
Serotonin
and Depression: A Disconnect between the Advertisements and the
Scientific Literature, by Jeffrey R. Lacasse and
Jonathan Leo.
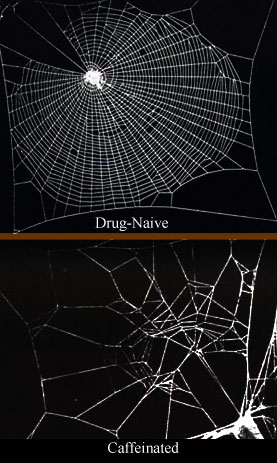
Illustration:
Margaret Shear, Public Library of Science
I was surprised to see this, because it is, to me, a new twist on the
old theme. The authors do not imply that antidepressant
medication does not work; nor do they argue that psychopharmacology is
suspect.
To equate the impressive recent achievements of
neuroscience with support for the serotonin hypothesis is a mistake.
Rather, they argue that it is inappropriate for pharmaceutical
companies to base advertising campaigns upon the presumed link between
serotonin and depression.
In the US, the FDA monitors and regulates DTCA.
The FDA requires that advertisements “cannot be false or
misleading” and “must present information that is
not inconsistent with the product label” [27]. Pharmaceutical
companies that disseminate advertising incompatible with these
requirements can receive warning letters and can be sanctioned. The
Irish equivalent of the FDA, the Irish Medical Board, recently banned
GlaxoSmithKline from claiming that paroxetine corrects a chemical
imbalance even in their patient information leaflets [29]. Should the
FDA take similar action against consumer advertisements of SSRIs?
Curiously, the authors devote several paragraphs to debunking the
serotonin hypothesis, even though, in my opinion, their purpose could
have been served with one or two citations. What is even more
curious is that they do not go on to draw a specific conclusion that
answers the question they pose: they never answer directly the question
about whether the FDA should take action against the pharmaceutical
companies that refer to the serotonin hypothesis in their
advertisements.
In fact, they do make a good case against the pharmaceutical companies,
and I happen to agree. It appears to be true, based upon
their argument, that pharmaceutical companies are not following FDA
regulations regarding DTC advertisements. Moreover, the
authors make several other good points, such as this one:
Patients who are convinced they are suffering from a
neurotransmitter
defect are likely to request a prescription for antidepressants, and
may be skeptical of physicians who suggest other interventions, such as
cognitive-behavioral therapy [48],
evidence-based or not.
I personally have spent a lot of time in the office, with patients,
trying to undo the misinformation contained in DTCA. It
bothers me that I have to do that. I would much rather spend
the time providing good education, not undoing bad education.
I would prefer to not have to deal with direct-to-consumer
advertising at all; but if we have to have it, companies really ought
to be held to the standards that exist to ensure balance and accuracy.






")

")



")



 What is
interesting about the TCA's effort is the way they are helping to
reduce predation of tenkiles. The local humans traditionally
have hunted the tenkile. The TCA has
What is
interesting about the TCA's effort is the way they are helping to
reduce predation of tenkiles. The local humans traditionally
have hunted the tenkile. The TCA has 




 :
Joseph j7uy5
:
Joseph j7uy5
{kind=link}